
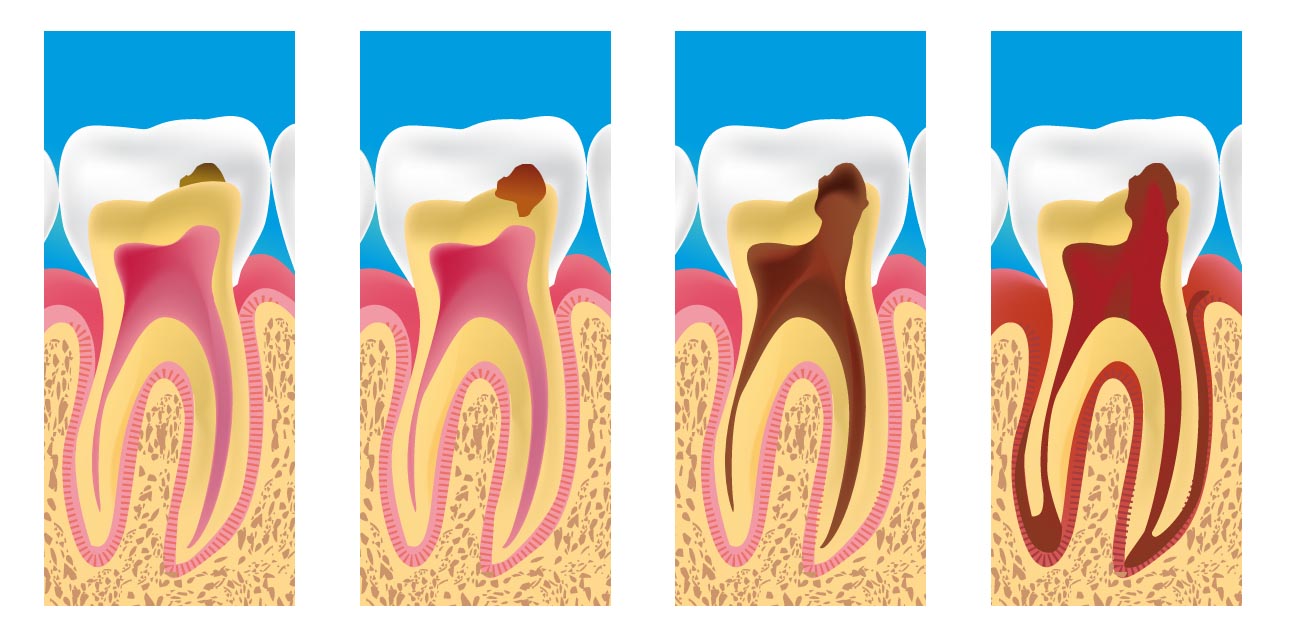
Dental caries, also known as tooth decay or cavity, is a disease where bacterial processes damage hard tooth structure (enamel, dentin, and cementum). These tissues progressively break down, producing dental caries (cavities, holes in the teeth). If left untreated, the disease can lead to pain, tooth loss, infection,... The presentation of caries is highly variable; however, the risk factors and stages of development are similar. Initially, it may appear as a small chalky area that may eventually develop into a large cavitation. Sometimes caries may be directly visible, however other methods of detection such as radiographs are used for less visible areas of teeth and to judge the extent of destruction. Tooth decay is caused by specific types of acid-producing bacteria that cause damage in the presence of fermentable carbohydrates such as sucrose, fructose, and glucose. Dental health organizations advocate preventive and prophylactic measures, such as regular oral hygiene and dietary modifications, to avoid dental caries
Prevention
Personal hygiene care consists of proper brushing and flossing daily. The purpose of oral hygiene is to minimize any etiologic agents of disease in the mouth. The primary focus of brushing and flossing is to remove and prevent the formation of plaque. Plaque consists mostly of bacteria. As the amount of bacterial plaque increases, the tooth is more vulnerable to dental caries when carbohydrates in the food are left on teeth after every meal or snack. A toothbrush can be used to remove plaque on accessible surfaces, but not between teeth or inside pits and fissures on chewing surfaces. When used correctly, dental floss removes plaque from areas which could otherwise develop proximal caries. Other adjunct hygiene aids include interdental brushes, water picks, and mouthwashes.
However oral hygiene is probably more effective at preventing gum disease than tooth decay. The brush and fluoride toothpaste have no access inside pits and fissures, where chewing forces food to be trapped. (Occlusal caries accounts for between 80 and 90 percent of caries in children (Weintraub, 2001). The teeth at highest risk for carious lesions are the first and second permanent molars.)
Professional hygiene care consists of regular dental examinations and cleanings. Sometimes, complete plaque removal is difficult, and a dentist or dental hygienist may be needed. Along with oral hygiene, radiographs may be taken at dental visits to detect possible dental caries development in high risk areas of the mouth.
Sealant
 The use of dental sealants is a means of prevention. A sealant is a thin plastic-like coating applied to the chewing surfaces of the molars. This coating prevents food being trapped inside pits and fissures in grooves under chewing pressure so resident plaque bacteria are deprived of carbohydrate that they change to acid demineralisation and thus prevents the formation of pit and fissure caries, the most common form of dental caries. Sealants are usually applied on the teeth of children, shortly after the molars erupt. Older people may also benefit from the use of tooth sealants, but their dental history and likelihood of caries formation are usually taken into consideration..
The use of dental sealants is a means of prevention. A sealant is a thin plastic-like coating applied to the chewing surfaces of the molars. This coating prevents food being trapped inside pits and fissures in grooves under chewing pressure so resident plaque bacteria are deprived of carbohydrate that they change to acid demineralisation and thus prevents the formation of pit and fissure caries, the most common form of dental caries. Sealants are usually applied on the teeth of children, shortly after the molars erupt. Older people may also benefit from the use of tooth sealants, but their dental history and likelihood of caries formation are usually taken into consideration..
Symptoms
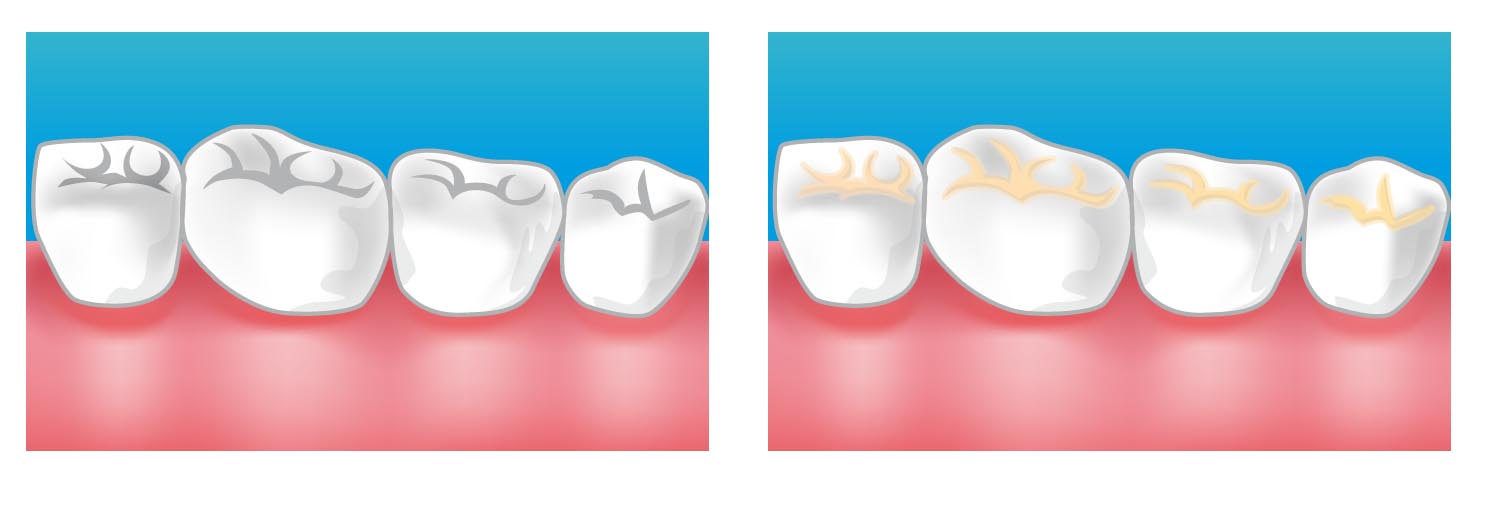
A person experiencing caries may not be aware of the disease. The earliest sign of a new carious lesion is the appearance of a chalky white spot on the surface of the tooth, indicating an area of demineralization of enamel. This is referred to as incipient decay. As the lesion continues to demineralize, it can turn brown but will eventually turn into a cavitation ("cavity"). Before the cavity forms, the process is reversible, but once a cavity forms, the lost tooth structure cannot be regenerated. A lesion which appears brown and shiny suggests dental caries were once present but the demineralization process has stopped, leaving a stain. A brown spot which is dull in appearance is probably a sign of active caries.
Treatment 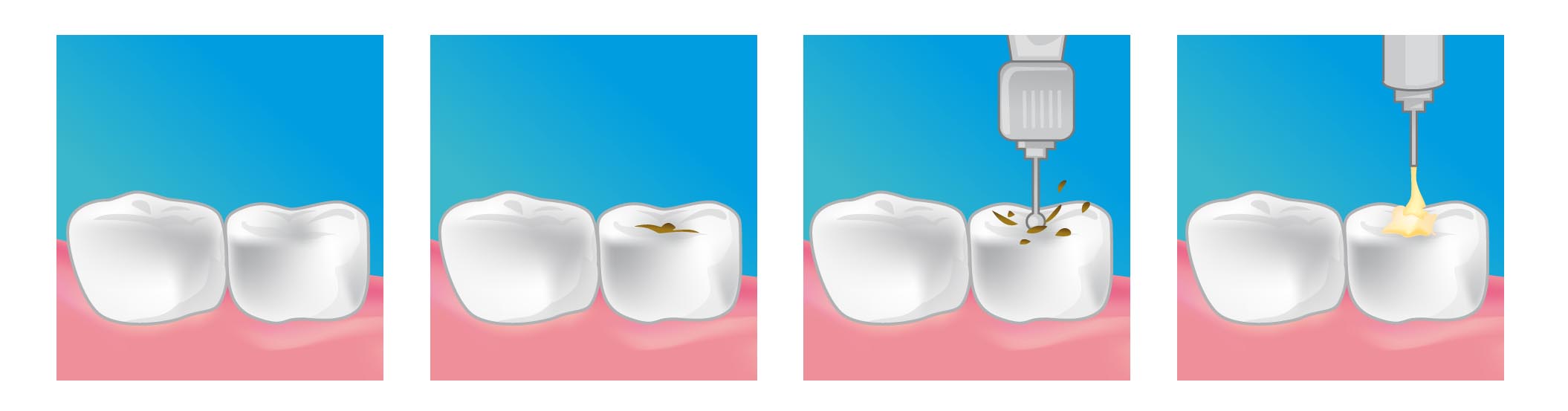
Restorative materials include dental amalgam, composite resin, porcelain, and gold. Composite resin and porcelain can be made to match the color of a patient's natural teeth and are thus used more frequently when aesthetics are a concern. Composite restorations are not as strong as dental amalgam and gold; some dentists consider the latter as the only advisable restoration for posterior areas where chewing forces are great. When the decay is too extensive, there may not be enough tooth structure remaining to allow a restorative material to be placed within the tooth. Thus, a crown may be needed. This restoration appears similar to a cap and is fitted over the remainder of the natural crown of the tooth. Crowns are often made of gold, porcelain, or porcelain fused to metal.